Sweden
- Federica Andreoni
- Mohammad Al-Ubaydli
Country’s healthcare system in a nutshell
The Swedish healthcare system is decentralised: the 21 regions are responsible for care provision and can decide whether to contract public or private providers. The system is publicly funded, covering all the people resident in Sweden, regardless of their nationality. 85% of its financing originates from regional taxes, complemented by direct federal government transfers.
The system is structured into three administrative tiers :
The national government establishes health and medical care principles and guidelines, setting policy priorities through laws, ordinances, or agreements with the Swedish Association of Local Authorities and Regions (SKR).
The 21 regions organize health and medical care to ensure universal access.
The 290 municipalities handle care for the elderly, individuals with physical and mental disabilities, post-therapy support, and school health care.
Two important pillars of the eHealth strategy in Sweden are E-hälsomyndigheten (eHM), which is the Swedish eHealth Agency, and Inera AB, a company owned by all Regions, Municipalities and Swedish Association of Local Authorities and Regions (SKR). These two are distinct entities that occasionally collaborate.
The Swedish eHealth Agency is a government entity dedicated to digitalizing and enhancing the exchange of information among patients, the healthcare system, and pharmacies within the country. The Agency is in fact focused on e-prescriptions, and it was also tasked by the Ministry of Social Welfare for the creation of the Covid certification during the pandemic. Its responsibilities are:
Carrying out the government's e-health initiatives.
Storing digital prescriptions from doctors and forwarding them to pharmacies.
Offering Medicine Check service. This allows patients to view information about their prescriptions and whether they are eligible for the high-cost protection card (if patients receive this, they don’t pay for medicines for a set period).
Collecting information about the quantities of and which medicines have been sold in Sweden.
Offering the Electronic Expert Support service to help pharmacies check whether prescription medicines work together.
(Welcome to the Swedish eHealth Agency, 2024)
Inera is a “digitization company that, on behalf of municipalities and regions, contributes to the development of welfare.” Inera’s eHealth strategy is based on:
National Patient Overview (NPÖ), which allows healthcare providers to see and share patient information securely across different regions.
1177 and Journalen, which are designed to offer support and engage citizens.
The remainder of this chapter will focus on 1177, with particular emphasis on Journalen, which serves as Sweden's national Personal Health Record (PHR).
Public vs private

The pink column refers to the public expenditure as a % of the country’s total healthcare expenditure. The blue dot is the country’s expenditure on health per capita, expressed in international dollars at purchasing power parity.
The national PHR
History
Inera AB, owned by the regions, municipalities and the Swedish Association of Local Authorities and Regions (SALAR), manages the national patient portal 1177.se (Cijvat, Cornet and Hägglund, 2021). The portal comprises three key components: a telephone advice service (1177 on the phone), a web-based information platform (1177.se on the web), and a Personal Health Record. The latter, accessible through e-ID authentication, is called Journalen and serves as the national Personal Health Record in Sweden (Hägglund, Blease & Scandurra, 2020).
Journalen integrates Electronic Health Record (EHR) information from various systems used by Swedish healthcare organisations through a national health information exchange platform. Initially launched as a project in the Uppsala region, its success inspired other regions, that requested to adopt it. As a result of this, Uppsala transferred the project to Inera for national management. The first region connected to this infrastructure in 2012, with the final joining in 2018. Despite this widespread adoption, features still vary depending on the region and on the healthcare provider (Hägglund, Scandurra 2022). Today, Journalen serves as a centralised access point, connecting EHR systems across all 21 regions in Sweden.
eHealth is deeply embedded in Sweden's healthcare system, with annual investments of around $1.22 billion in healthcare IT across all regions. Electronic health record solutions are universally adopted, with 99% of prescriptions issued electronically. The COVID-19 pandemic further accelerated the adoption of digital health services, with digital consultations doubling in 2020, representing 11% of all medical appointments
In collaboration with the Swedish Association of Local Authorities and Regions (SALAR), the Swedish government has outlined a vision for its national eHealth strategy. By 2025, the country aims at becoming a global leader in utilising digitalisation and eHealth to enhance health and welfare, while promoting individuals' independence (International Trade Administration, U.S. Department of Commerce, 2023).

{kind=link}
The following image illustrates in more detail the structure of Sweden's healthcare data exchange.
At the bottom are the source systems, which include local electronic health record (EHR) systems. These feed data into the larger regional databases.
At the centre of the diagram is the National Service Platform (NTjP), which serves as the hub for data exchange. It connects different healthcare providers and systems across Sweden. Information such as lab results, vaccinations, and diagnoses flows into the NTjP via APIs from regional databases and other authorised systems.
On the left, there is a blue box representing an electronic directory that contains data about healthcare organisations and personnel, such as clinicians, operating across the country.
At the top of the diagram are consumer platforms like 1177 and Journalen, which provide patients with access to their health information.
On the bottom left, some source systems represent private healthcare providers. These providers have their own EHR systems but cannot directly connect to the NTjP because they are private. However, their tech company (or a third-party company) can apply to become an agent for Inera. Agents connect systems to Inera's infrastructure and ensure the technical requirements are met for healthcare providers to use Inera's services.
Agents themselves do not use the services but enable healthcare providers to send data to platforms like Journalen. Importantly, private providers can only send data for services funded by tax money, so self-funded procedures (e.g., cosmetic surgery) are excluded.
Being an agent typically costs more than regional access, but many regions require this connection when contracting private providers. Additionally, agents have limited access to certain services.
Features
Note from the author: the bibliography for this section is from 2018, and we were unable to locate more recent information.
Within the Journalen system, patients can access the following:
Medical notes from the EHRs, from all healthcare professionals and connected healthcare providers (both public and private) who have agreed to give access.
A list of prescribed medications.
Laboratory results.
Warnings.
Diagnoses.
Maternity care records.
Referrals.
Vaccination records.
In some regions, users can also access a log function, allowing them to see who has viewed their record.
Challenges and areas for improvement
One significant challenge for Journalen is data fragmentation, as various Electronic Health Record (EHR) systems are in use across the country. To address the challenge of consolidating EHR data for patients, Sweden has, as detailed above, implemented a national Health Information Exchange platform. Despite these efforts, challenges remain in achieving a comprehensive overview of health data. Variability in information accessibility among care providers—due to differing policies and regulations—results in a fragmented patient view, depending on the location, timing, and purpose of seeking treatment. This issue is closely tied to the difficulty in agreeing on a national regulatory framework for patients’ direct access to their health information.
Resistance to change among healthcare professionals also poses challenges. Many professionals are concerned about how the system might impact their work. Key worries include an increase in workload, as more time may be required to explain EHR contents and address patient queries. Some professionals also fear that patient access to EHRs could lead to misunderstandings, misinterpretations, and conflicts, potentially causing unnecessary anxiety for patients (Hägglund, 2017).
A 2022 survey on the usability of the Swedish Personal Health Record highlighted several additional concerns:
Due to regional adaptations of the national regulatory framework for Patient-Accessible Electronic Health Records (PAEHR), different regions offer distinct features and provide varying levels of health information to patients.
Some regions did not retroactively provide access to health information; records only include data from the date the region launched the portal.
Many regions impose restrictions on patient access to specific clinical data, such as mental health records. Some respondents felt discriminated against due to the limited access to their mental health information.
When a child turns 13, parents lose access to the child’s record, yet the child cannot access their own record until they turn 16. This results in a three-year period where neither the parent nor the child can view the health record.
The platform lacks a messaging feature, preventing patients and healthcare professionals from communicating with each other remotely.
(Hägglund and Scandurra, 2022)
The following table, from Cijvat, Cornet and Hägglund, 2021 (Table 4), shows “Barriers on the local implementation level”:
Category | Sweden | Netherlands |
|---|---|---|
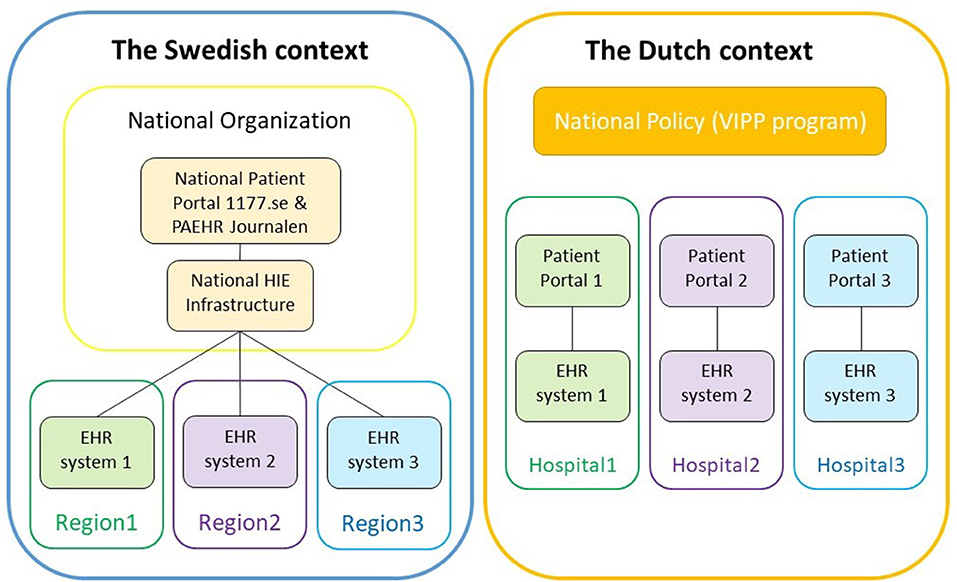
Systems and suppliers | Technical limitations of systems. High costs for connecting small EHR systems. Testing prior to implementation is necessary. Difficult requisites for connecting to the HIE. | Limitations in choice and possibilities of systems. Large dependency on software suppliers. Alignment of systems necessary but difficult. Systems and suppliers determine the achievement of VIPP (VIPP programme is an initiative in the Netherlands designed to enhance the exchange of information between patients and healthcare professionals). |
Social and organisational | Resistance and fears from physicians. Changing healthcare providers' routines, workflows and attitudes. | Physicians' reluctance, resistance and fears. Changing healthcare providers' political status and workflow. Effects on hospitals' culture and work processes. Concerns for patients' confusion, questions, and fears. Gradual implementation is necessary to keep physicians on board. |
Resources | High costs for connecting to HIE. Time-consuming decision-making due to flexibility in the national regulatory framework. | VIPP requires a lot of human work. Human work leads to high costs. Too little time to make VIPP’s deadlines. |
Policies, laws and regulations |
| Some VIPP goals are difficult to accomplish. Strict privacy regulations are not in patients' interests. Strict security rules impede user-friendliness. |
Governance | A gradual approach is necessary to get all stakeholders on board. Flexibility in choosing EHR systems in some countries but only one supported. | Gradual implementation to keep physicians on board. VIPP has no or low-priority. |
The following table, from Cijvat, Cornet and Hägglund, 2021 (Table 3), shows “Barriers on the national level”:
Category | Sweden | The Netherlands |
|---|---|---|
Systems and suppliers | Authentication methods. | Difficulties in measuring hospitals' progress |
Social and organisational | Resistance and fears from physicians. | - |
Resources | Financing the development of Journalen. Too little time to take precautions for physicians' resistance. | - |
Policies, laws and regulations | Include electable rules to make progress. Electable rules caused confusion and inequality for users. Giving patients direct online access to records was illegal when Journalen was first introduced in 2002. | Challenging to define goals adequately for desired outcomes. Challenging to estimate reasonable usage percentages. Slow development of other national programs. |
Effects of barriers | Delays. Restrictions on information that is displayed. | Delays. |
Published outcomes - statistics
Unfortunately, we couldn’t find any statistics about the use of the Swedish PHR. If you have access to this information or can put us in touch with someone who has, please contact us at book@phr4gov.org
Screenshots
Unfortunately, we couldn’t find any screenshots of the Swedish PHR. If you have access to this information or can put us in touch with someone who has, please contact us at book@phr4gov.org
Bibliography
Cijvat, C.D., Cornet, R. and Hägglund, M., 2021. Factors influencing development and implementation of patients' access to electronic health records—a comparative study of Sweden and the Netherlands. Frontiers in Public Health, 9, p.621210. (online). Available at: Frontiers | Factors Influencing Development and Implementation of Patients' Access to Electronic Health Records—A Comparative Study of Sweden and the Netherlands (accessed 3 May 2023).
eHealth in Sweden, n.d. GNIUS. Edited by Délégation au numérique en santé (Ministerial delegation for Digital Health). Available at: https://gnius.esante.gouv.fr/en/international-digital-health-systems/ehealth-in-sweden (accessed 3 May 2023).
Hägglund, M., 2017. Electronic health records in Sweden—how can we go from transparency to collaboration? Thebmjopinion. (online) 23 June. Available at: Maria Hägglund: Electronic health records in Sweden—how can we go from transparency to collaboration? - The BMJ (accessed 2 August 2024).
Hägglund, M., 2020. Mobile access and adoption of the Swedish National Patient Portal. In: A. Värri et al., eds. Integrated Citizen Centered Digital Health and Social Care. The European Federation for Medical Informatics (EFMI) and IOS Press. Available at: https://www.diva-portal.org/smash/get/diva2:1509909/FULLTEXT01.pdf (accessed 3 May 2023).
Hägglund, M. and Scandurra, I., 2022. Usability of the Swedish accessible electronic health record: qualitative survey study. JMIR Human Factors, 9(2), p.e37192. (online) Available at: Usability of the Swedish Accessible Electronic Health Record: Qualitative Survey Study (accessed 3 May 2023).
Inera, 2024. Inera. Available at: Inera (accessed: 14 November 2024).
International Trade Administration, U.S. Department of Commerce, 2023. Sweden - Country Commercial Guide. (online) Available at: Sweden - eHealth (accessed 3 May 2023).
Moll, J., Rexhepi, H., Cajander, Å., Grünloh, C., Huvila, I., Hägglund, M., Myreteg, G., Scandurra, I. and Åhlfeldt, R.M., 2018. Patients’ experiences of accessing their electronic health records: national patient survey in Sweden. Journal of Medical Internet Research, 20(11), p.e278. (online) Available at: Patients’ Experiences of Accessing Their Electronic Health Records: National Patient Survey in Sweden (accessed 3 May 2023).
Welcome to the Swedish eHealth Agency, n.d. eHälsomyndigheten. Available at: https://www.ehalsomyndigheten.se/languages/english/welcome-to-the-swedish-ehealth-agency/ (accessed 3 May 2023).
Back: Catalonia / Next: Türkiye